Esophageal Pseudo-Dyspnea.
- Jun 30, 2025
- 7 min read
Updated: Aug 10, 2025
A newly described condition by Hanna Saadah, MD, FACP. Republished with permission from the Oklahoma County Medical Society Bulletin, July/August 2023.
To discuss a complex neurological-cardiopulmonary-gastrointestinal disorder, I begin by defining two clinical types of dyspnea:
A) Objective dyspnea, results from inadequate oxygen delivery, limits physical activity, and worsens with exercise. Disorders that cause objective dyspnea include obesity and diseases of the heart, lungs, blood, blood vessels, and others.
B) Subjective dyspnea, occurs despite adequate oxygen delivery, does not limit physical activity, and does not worsen with exercise. Disorders that are known to cause subjective dyspnea are mostly psychogenic and include anxiety, panic, phobias, hyperventilation syndrome, sighing dyspnea syndrome, and others.
C) Esophageal Pseudo-Dyspnea, the term I have chosen for this disorder, is another subjective dyspnea, but it is not psychogenic.
Case Reports
HS: As a third-year medical student in 1969, I suffered from a pervasive feeling of shortness of breath, which was ameliorated by jogging. I had no cough, wheezing, heartburn, tachypnea, or chest pain, but I did have a persistent urge to take in frequent deep sighs, which did not appease my shortness of breath. That annoying shortness of breath persisted for several months, was not influenced by position, but did improve briefly with food. A medical investigation yielded no diagnosis, and no treatment was offered. As a fourth-year medical student, I happened to self-treat an isolated episode of heartburn with liquid antacid and noticed that it also relieved my shortness of breath. After taking the antacid several times daily for a few weeks, my shortness of breath abated and has not recurred.
JG: A 74-year-old man who, on January 5, 2022, complained of a new, pervasive feeling of shortness of breath for several weeks. The shortness of breath gets worse when he lies down, improves when he walks or becomes physically active, causes him to take in frequent deep sighs, and makes him feel anxious and panicked. He had normal vital signs, no tachypnea, and no cardiopulmonary or gastrointestinal symptoms. His laboratory tests and his physical examination were normal, but he had gained ten pounds to a weight of 223 lbs. during Christmas.
Based on my long-term familiarity with this disorder, I attributed his subjective dyspnea to silent esophagitis secondary to silent gastroesophageal reflux. I reassured him because he had suffered from chronic anxiety-panic and had been on treatment with Buspirone for several years. After educating him, I gave him a therapeutic trial of liquid Maalox, liquid Gaviscon, Omeprazole 20 mg twice daily, and acid reflux precautions. He returned nine weeks later and reported that his subjective dyspnea had resolved after six weeks of treatment and that he had stopped taking Maalox, Gaviscon, and Omeprazole. He also related that his chronic anxiety-panic that were rekindled by his dyspnea had also remitted. He returned five months, nine months, and one year later, and was still free of subjective dyspnea and anxiety-panic.
JD: A 74-year-old man who, on June 3, 2021, complained of a new feeling of shortness of breath for several weeks. The shortness of breath comes when he is sitting, especially after meals, and it gets worse when he lies down. He takes frequent deep sighs, but they fail to temper his shortness of breath. When he is active, doing construction work, his shortness of breath disappears. He had been on long-term Omeprazole 20 mg/day for chronic gastroesophageal reflux. His laboratory tests, vital signs, and physical examination were normal. He had no tachypnea, cough, heartburn, or other gastrointestinal symptoms, but he had gained about 10 pounds to a weight of 159.3 lbs.
His chronic anxiety-panic had been under good control with Clonazepam and were unaffected by his shortness of breath. Based on my long-term familiarity with this disorder, I attributed his subjective dyspnea to silent esophagitis secondary to silent gastroesophageal reflux and increased his Omeprazole to 20 mg twice daily, added 45 cc of liquid Maalox PRN for shortness-of-breath episodes, and instructed him in reflux precautions. He returned after three weeks and reported that his shortness of breath is coming only after dinner and that he is taking his Omeprazole in the morning and at bedtime but without food.
I educated him that Omeprazole works best when taken before food and asked him to take his Omeprazole before dinner and to eat a small breakfast before taking it in the morning. He returned nine months later and reported that his shortness of breath was under control, that he was still taking Omeprazole twice daily, and that he’s able to abort shortness-of-breath episodes with liquid Maalox. He returned a year later and reported that his shortness of breath has totally disappeared, that he continues to take Omeprazole 20 mg twice daily, and that his anxiety-panic are still well controlled with Clonazepam.
He returned 18 months later and reported that his shortness of breath has been under perfect control for over a year with Omeprazole 20 mg twice daily, that it used to come daily, that it used to frighten him, and that he is still treating occasional heartburn episodes, which come without dyspnea. He returned 27 months later and reported that his shortness of breath and gastroesophageal reflux were in total remission.
Discussion
Since my personal experience in 1969, I had treated several patients with esophageal pseudo-dyspnea and posted my observations on my medical blog on 10/15/2012 under the title False Shortness of Breath (Pseudodyspnea). Last year, I shut down my web, but that same medical blog article was republished by The Monthly magazine, Issue 125, December 2012.
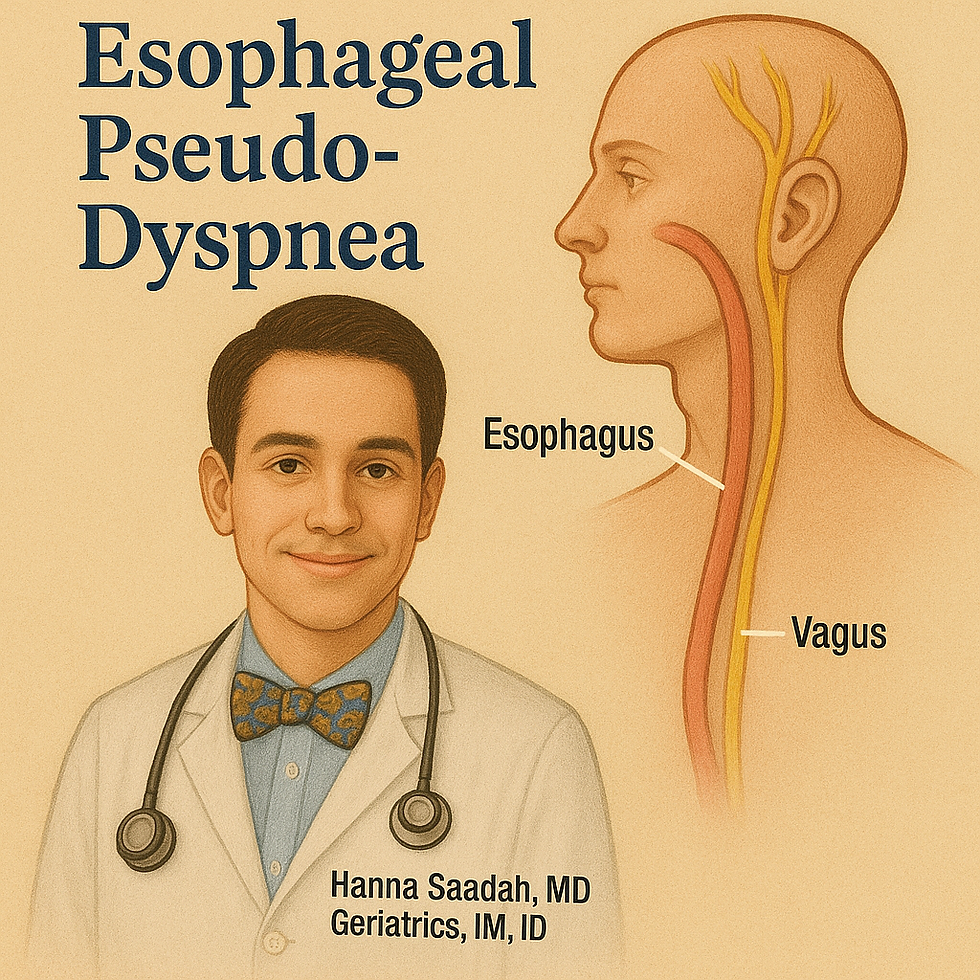
Understanding the vagal nerve’s ramifications is key to understanding esophageal pseudo-dyspnea. The vagus nerve (cranial nerve X) has four medullary nuclei: two nuclei (Nucleus of the Solitary Tract and Spinal Nucleus of the Trigeminal nerve) receive afferent input from the gastrointestinal, cardiac, pulmonary, and pharyngo-laryngeal systems. Two nuclei (Dorsal Motor Nucleus and Nucleus Ambiguus) send efferent output to modulate these four systems. The esophageal and the pulmonary vagal plexuses, which send afferent input to the Nucleus of the Solitary Tract, sense chemicals, inflammation, pressure, pain, stretch, temperature, and osmotic pressure. The Nucleus of the Solitary Tract transmits the received sensory information to multiple brain regions for interpretation. The vagal nerve efferent output from the Dorsal Motor Nucleus and Nucleus Ambiguus regulate respiration, feeding, heart rate, blood pressure, vascular resistance, and airway diameter.
Chemical and inflammatory information from the lower esophagus is transmitted by the esophageal plexus, along afferent vagal fibers, to the Nucleus of the Solitary Tract—the same nucleus that also receives afferent fibers from the pulmonary plexus. This nucleus may provide a hub for the esophageal-pulmonary connection.
It is conceivable that when the Nucleus of the Solitary Tract transmits the received information from the lower esophagus and from the lungs to multiple brain regions, the brain may misinterpret the information as dyspnea, which can trigger deep sighing. This referred esophageal-pulmonary feeling of shortness of breath is reminiscent of the referred left-arm pain of angina pectoris and the referred right-shoulder pain of gallbladder disease.
Experimentally, bronchoconstriction and cough can be induced by acid infusion into the distal esophagus—via a vagally mediated reflex—which is another manifestation of the esophageal-pulmonary connection.
Moreover, adverse effects of therapeutic vagal nerve stimulation include dyspnea in 8%, cough in 8%, and an increase in apnea/hypopnea episodes in patients who already have obstructive sleep apnea.
Lower esophageal sphincter tone is regulated by the Dorsal Motor Nucleus of the vagus nerve. Transient relaxations of the lower esophageal sphincter are responsible for 63–74% of acid reflux episodes. Chronic cough can be a manifestation of gastroesophageal reflux without aspiration, and a therapeutic trial of acid suppression by proton pump inhibitors can confirm that diagnosis. In asthmatics, gastroesophageal reflux without aspiration can trigger asthma attacks that result from increased vagal tone and heightened bronchial reactivity.
Episodic dyspnea that does not interfere with daily activities also occurs in 60–70% of healthy pregnancies and is more pronounced during the first trimester than the third. The mechanism of the episodic dyspnea of pregnancy is not known and no therapy has yet been advanced. Perhaps a therapeutic trial with liquid antacids may provide a diagnosis and a treatment.
On palliative-care floors, agonizing dyspnea is treated with oxygen, morphine, and benzodiazepines. Since acid reflux is common in terminally ill, recumbent patients who are on medications that relax the lower esophageal sphincter, such as morphine, a therapeutic trial with liquid antacid may provide additional relief.
The five clinical features of esophageal pseudo-dyspnea, as exemplified by these three case reports, are:
The perceived feeling of shortness of breath is prolonged (spanning several weeks), is accompanied by frequent deep sighs, and is not accompanied by hyperventilation, tachypnea, cough, or heartburn.
The perceived shortness of breath does not limit physical activity and does not worsen with exercise.
The perceived shortness of breath resolves with intense anti-acid therapy and reflux precautions.
The diagnosis of esophageal pseudo-dyspnea is clinical and is confirmed by response to intensive anti-acid therapy and reflux precautions. There are no reliable diagnostic tests; upper endoscopy reveals a low prevalence of esophagitis. Moreover, the absence of gastrointestinal symptoms renders the request for endoscopy unjustifiable.
Preexisting anxiety-panic can be rekindled by esophageal pseudo-dyspnea and remit when the dyspnea resolves. Dyspnea fear is major among those with asthma, COPD, anxiety, panic, and phobias, but is less intense among normal subjects.²
Conclusion
Esophageal pseudo-dyspnea is common and causes apprehension, suffering, and expense, as judged by the number of calls I continue to receive, the thousands of hits my blog article⁵,⁶ has received, and the pseudo-dyspnea internet chatter that is still ongoing.¹⁴The afferent vagal fibers of the esophageal plexus have a much higher sensitivity for reflux esophagitis than endoscopes.¹¹ Wasting effort and expense on low-yield investigations is counterproductive. The best diagnostic test is still a therapeutic trial with intense acid suppression and reflux precautions.
Conflict of Interest Statement
The main author Dr. Saadah has not reported any conflict of interest.
References
Gruber C, Lehmann C, Weiss C, Niggemann B. Somatoform respiratory disorders in children and adolescents—Proposals for a practical approach to definition and classification. Pediatr Pulmonol. 2012;47:199–205.
Carr RE, Lehrer PM, Hochron SM. Panic symptoms in asthma and panic disorder: A preliminary test of the dyspnea-fear theory. Behav Res Ther. 1992;30:251–261.
Kara MZ, Basaran AE. Psychological profiles, quality of life, and parental attitudes in children with sighing dyspnea. Clin Child Psychol Psychiatry. 2022;27:769–781.
Saadah H. Letter to the editor. Oklahoma County Medical Society Bulletin. 2013;September/October.
Saadah H. False Shortness of Breath (Pseudodyspnea). [Internet]. Available from: http://hannasaadah.com/blog/medical/false-shortness-of-breath-pseudo-dyspnea-december-12/
Saadah H. False Shortness of Breath. The Monthly Magazine [Beirut, Lebanon]. Issue 125, December 2012. (Electronic copy available upon request: hannasaadah@hotmail.com).
Yuan H, Silberstein SD. Vagus nerve and vagus nerve stimulation, a comprehensive review: Part I. Headache. 2016;56:71–78.
Schachter SC. Vagus nerve stimulation therapy for the treatment of epilepsy. UpToDate. 2022.
Harding SM. Gastroesophageal reflux, asthma, and mechanisms of interaction. Am J Med. 2001;111(8A):8S–12S.
Irwin RS, Madison JM, Fraire AE. The cough reflex and its relation to gastroesophageal reflux. Am J Med. 2000;108(4A):73S–78S.
Gurski RR, Da Rosa AR, Do Valle E, De Borra MA, Valiati AA. Extraesophageal manifestations of gastroesophageal reflux disease. J Bras Pneumol. 2006;32(2):150–160.
Kahrilas PJ. Complications of gastroesophageal reflux in adults. UpToDate. 2022.
Goland S, et al. Shortness of breath during pregnancy. Clin Cardiol. 2015;38:598–603.
[Video link on pseudo-dyspnea]. Available from: https://youtu.be/k9Of97zpyuA

Comments